Microneedling for Hair Growth: What the Evidence Says
A conservative, evidence-based guide to microneedling for hair growth, minoxidil timing, safety, and progress tracking.
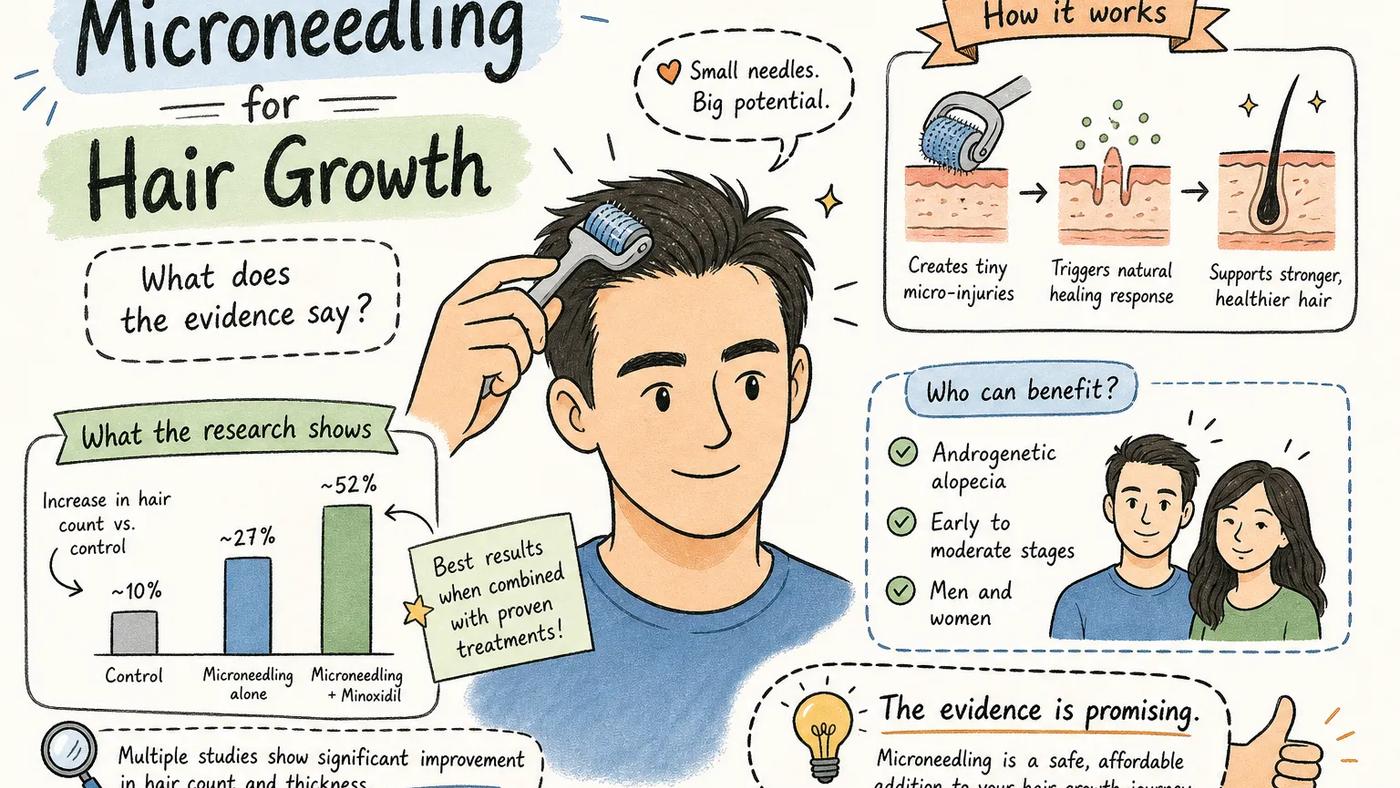
Direct answer: microneedling has real clinical evidence as an adjunct for androgenetic alopecia, especially when paired with minoxidil, but it is not a standalone cure and it is not something to do over an inflamed or infected scalp. This draft is educational, not medical advice.
Founder note: I would only judge a microneedling routine from repeatable photos, session dates, reactions, and a long enough review window. Folicle exists because guessing from a camera roll made my own hair-loss tracking messier than it needed to be.
Microneedling hair growth strategies have moved from a dermatology clinic niche to a routine that men and women are running on their own bathroom counters every week. The appeal is obvious: create controlled micro-injuries, trigger the body's healing response, and coax dormant follicles back into growth. The biological rationale is genuinely sound. What's less clear is whether the clinical evidence justifies the hype, and whether most people running a dermaroller across their scalp are actually doing it in a way that produces results.
This guide covers the full picture: the cellular mechanism behind microneedle therapy for hair loss, what randomized controlled trials actually measured and found, the right needle depths and session frequencies, the combination therapies worth adding versus the ones that aren't proven yet, what a safe at-home protocol looks like, and who should skip this treatment entirely. One more thing gets covered at the end: how to track whether it's working. That part matters more than most people realize, because slow hair regrowth measured with inconsistent phone photos isn't being measured at all.
Why scalp microneedling triggers hair regrowth in the first place
The mechanism behind dermarolling for hair isn't mysterious, but it is specific. Understanding it explains why protocol details, needle depth, frequency, timing, aren't arbitrary preferences. They're the variables that determine whether you're triggering a meaningful biological response or just irritating your scalp for no gain.
The wound-healing cascade and what it releases
When a microneedle punctures the dermis, it triggers the same wound-healing cascade your body runs for any controlled injury: platelets aggregate at the site, and the healing process releases a surge of growth factors. Research on scalp microneedling specifically demonstrates upregulation of VEGF (vascular endothelial growth factor) and activation of the Wnt signaling pathway. VEGF is particularly significant because it drives angiogenesis, the formation of new blood vessels, which improves the oxygen and nutrient delivery that active follicles need. PDGF (platelet-derived growth factor) and EGF (epidermal growth factor) are biologically plausible contributors based on wound-healing physiology, though they haven't been directly measured as outcomes in the published scalp microneedling trials. The key distinction from random scalp trauma is the controlled, repeatable nature of the injury. Microneedling creates a predictable wound density at a consistent depth, which produces a reproducible healing response. That predictability is what makes the protocol matter.
Stem cell and follicle activation via the Wnt pathway
Beyond the platelet response, the research points to something more targeted: microneedling upregulates Wnt3a, Wnt10b, and β-catenin, the canonical Wnt/β-catenin signaling pathway directly involved in hair follicle regeneration, shaft growth, and anagen initiation. Micro-injuries near the bulge region of the hair follicle, where follicular stem cells reside, stimulate those stem cells toward the anagen (active growth) phase from the telogen (resting) phase. That shift is the biological goal of the entire protocol. Collagen induction therapy, another name for the same process, also improves dermal thickness and local blood supply around follicles over time, creating a better microenvironment for sustained growth.
Why androgenetic alopecia is a plausible target
In androgenetic alopecia, the mechanism of damage is DHT-driven follicular miniaturization: follicles progressively shrink, spend less time in anagen, and produce thinner, shorter hairs until they stop producing visible hair at all. Growth factor stimulation via microneedling works in the opposite direction, pushing follicles back toward anagen and improving the vascular environment that sustains active growth. This is why scalp microneedling is positioned as a logical adjunct rather than a standalone cure. Microneedling doesn't block DHT. But it does address the follicular environment in a way that complements treatments that do, particularly minoxidil. That complementary logic is exactly what the clinical trials set out to test.
Microneedling hair growth: what randomized clinical trials actually show
The biological mechanism is plausible, but mechanism alone doesn't determine whether a treatment works clinically. What the controlled trial data shows is more convincing than most people expect, with some important caveats about how the evidence is structured.
The head-to-head RCT: microneedling vs. minoxidil alone
The most cited randomized, single-observer blinded study compared microneedling combined with topical minoxidil against minoxidil alone in androgenetic alopecia patients. The combination group produced a mean increase of 12.52 new hairs per square inch versus 1.89 hairs per square inch in the minoxidil-only group (P < 0.0001). A separate earlier trial measuring outcomes at 12 weeks showed mean hair count increases of 91.4 in the microneedling group versus 22.2 in the control group (P = 0.039). Patient-reported satisfaction also favored the combination arm in both studies. These aren't marginal differences. A four-to-six-fold advantage in hair count over monotherapy is a clinically meaningful signal, not a rounding error.
The 2025 meta-analysis: 13 trials, 696 patients
The pooled evidence from a systematic review and meta-analysis of 13 randomized clinical trials involving 696 patients confirmed the direction of the individual studies. Combined microneedling therapy showed a pooled mean difference of 18.11 for hair density and 2.50 for hair diameter (95% CI 0.99 to 4.02, P = 0.001) compared with monotherapy or control conditions. Physician-rated efficacy also significantly favored the combination arms. The safety profile across those 13 trials was comparable to monotherapy, with no serious adverse events reported across the combined study populations. That's the kind of meta-analytic signal that moves a treatment from "promising" to "evidence-supported adjunct, especially when a clinician agrees it fits the pattern."
Where the evidence has real gaps
The strongest evidence is concentrated in androgenetic alopecia, specifically the microneedling-plus-minoxidil combination. The data for microneedling as a standalone therapy, without any adjunct, is weaker. Evidence for other hair loss types, including alopecia areata and telogen effluvium, is thinner and more heterogeneous. Honest framing matters here: microneedling for hair regrowth is best framed as an evidence-supported adjunct for androgenetic alopecia treated with minoxidil. It has not earned the title of standalone cure, and it hasn't been rigorously validated across the full spectrum of hair loss diagnoses. Knowing that distinction determines whether it's worth adding to your routine.
Microneedling hair growth: choosing the right needle depth for your scalp
Needle depth is one of the two most practical questions people have when starting a scalp needling protocol, and it's where the assumption that "deeper is better" gets people into trouble. The clinical data on depth is more nuanced than most guides acknowledge.
The 0.5 to 1.5mm range and what each depth does
Depths in the 0.5 to 0.6mm range reach the upper dermis, which is enough to enhance topical absorption and trigger a mild growth factor response with lower post-treatment redness and irritation. The 1.0 to 1.2mm range reaches the mid-dermis and produces more robust growth factor activation, but also more pronounced redness and discomfort for several days. At 1.5mm, you're at the depth referenced most frequently in successful clinical studies, including several of the trials captured in the 2025 meta-analysis. Depths above 1.5mm have more theoretical risk of scarring and limited supporting evidence in scalp hair-loss trials; that range is not justified for most people using this protocol. For a practical, user-focused discussion on optimal microneedling lengths, see resources that review typical device settings and recommendations for scalp work.
Clinical findings on depth: deeper is not always better
One randomized study directly compared 0.6mm versus 1.2mm needle depths when combined with minoxidil, and the 0.6mm group produced superior hair count and hair thickness outcomes. This finding is counterintuitive but important: the deeper depth didn't outperform the shallower one in the key metrics. One explanation is that greater penetration increases inflammation and tissue disruption past the point of optimal healing response. There is no universal optimal depth that applies to every person because scalp skin thickness varies between individuals and across zones of the same scalp. That variability is a genuine argument for starting shallower and adjusting based on your response, not starting at 1.5mm simply because the literature supports that depth. For a detailed practical guide to needle lengths and their implications, see discussions from clinicians and hair-focused reviewers.
How device type changes what "depth" actually means
Dermarollers and automated dermapens don't behave identically at the same nominal depth setting. Rollers apply oblique penetration at an angle as the wheel turns, while pens deliver perpendicular, consistent penetration with each pass. Perpendicular penetration from an automated pen is generally more consistent and predictable than roller penetration at the same stated depth. For at-home scalp use, 24-pin or 36-pin cartridges at settings between 0.5mm and 1.5mm are most commonly referenced in practice-oriented clinical protocols. If you're using a fixed-depth roller, recognize that the actual dermal penetration will vary more than the needle length printed on the package suggests.
Session frequency and how long before results show
The second major practical question is how often to treat and how long to wait before evaluating results. Getting this wrong in either direction, treating too often or quitting too early, accounts for most protocol failures.
What the clinical evidence used as session frequency
The most frequently cited RCT protocol used biweekly sessions over 12 weeks, totaling six treatment sessions across the study period. Clinical practice guidelines for professional in-office treatment often suggest monthly sessions, reflecting the fact that professional treatments tend to use higher depths and intensities than at-home protocols. The appropriate frequency depends on three variables: device type, needle depth, and whether you're treating at home or in a clinical setting. A 0.5mm roller used at home every two weeks sits at a very different risk level than a 1.5mm dermapen session in a dermatologist's office once a month, and conflating those two frequency recommendations causes problems in both directions.
The minimum timeline to evaluate results honestly
Hair follicle cycling means structural changes at the follicle level won't translate into visible new growth for 8 to 16 weeks at minimum. The 12-week mark is the standard endpoint in most research trials. In clinical practice, practitioners commonly observe that a full microneedling protocol takes 4 to 6 months to fully manifest as visible density change, though this timeframe isn't yet precisely quantified in trial data. The most common protocol failure is quitting at the 6-to-8-week mark because nothing appears to have changed, before the biological response from your first sessions has had time to produce visible hair. Starting a protocol without committing to a 12-week minimum evaluation window is not a fair test of whether microneedling works for you specifically.
Signs that you're over-treating
Persistent redness that doesn't resolve within 5 days, tenderness that worsens rather than fades, pustules on the scalp, or flaking that spreads beyond the treated area are all signs that you're treating too frequently, too deeply, or both. The healing response that produces growth factors requires a recovery interval to complete. Treating again before the previous session's healing cycle finishes doesn't amplify results; it creates cumulative inflammation that can damage follicles rather than stimulate them. Rest intervals between sessions are not optional. A scalp that hasn't recovered from the last session should not be needled again regardless of what the schedule says.
Combining microneedling with minoxidil for a stronger routine
The best-evidenced combination in the hair loss literature is scalp microneedling paired with topical minoxidil. The data supporting this pairing is stronger than the data for any other combination, and the mechanism explains why.
Why this combination outperforms either treatment alone
Microneedling temporarily disrupts the stratum corneum barrier, creating microchannels that dramatically increase topical absorption. Minoxidil applied in the window following needling penetrates significantly more effectively than it would on intact skin. Beyond absorption, the growth factor release from the needling response works synergistically with minoxidil's vasodilatory mechanism: minoxidil expands blood vessels to improve scalp circulation while the wound-healing response simultaneously releases VEGF and Wnt pathway signals that push follicles toward anagen. Both the individual RCT data and the 2025 meta-analysis specifically favor this pairing over minoxidil monotherapy, with a four-to-six-fold improvement in hair count in the head-to-head trials. That synergy is the clinical basis for treating these as a unit rather than independent interventions.
The critical timing rule: when to apply minoxidil after a session
Applying minoxidil immediately after a microneedling session causes significantly increased burning, irritation, and risk of contact dermatitis. The disrupted skin barrier that makes minoxidil absorb more efficiently also allows it to absorb systemically at higher rates, and lets vehicle ingredients, propylene glycol, in most formulations, penetrate and irritate at levels they wouldn't on intact skin. Most dermatologist-facing guidance recommends waiting 24 hours post-session before applying minoxidil; some protocols extend this to 48 hours for individuals with more reactive skin. On non-needling days, minoxidil follows its normal schedule without any timing adjustment. That 24-hour gap is not a suggestion to skip a dose; it's a timing adjustment to protect the skin barrier while it starts recovering.
Logging the combination so you can see if it's working
A Folicle treatment log can record each microneedling session with date, needle depth, device, and any reactions, alongside your daily minoxidil applications, all linked to your weekly scalp photo timeline. The Hair Score can help you review changes across sessions, so when you compare the weeks before you added microneedling to the weeks after, you are looking at aligned photos and a consistent score trend, not a guess based on memory. Without that structure, the combination routine can produce noise you cannot interpret safely.
Other combination therapies: PRP, growth factors, and finasteride
The minoxidil pairing has the strongest evidence, but it's not the only combination discussed in the literature. Each of the others comes with a different evidence profile worth understanding before you add them to a protocol.
PRP and microneedling: stronger together in some cases
Platelet-rich plasma injections combined with scalp microneedling have shown improvements in SALT scores for alopecia areata and better hair density outcomes in androgenetic alopecia in several studies. The rationale is straightforward: PRP delivers a concentrated dose of growth factors directly into the follicular environment at the same time microneedling is stimulating the local healing response. The evidence is less robust and more heterogeneous than the minoxidil data, but it's directionally positive in the studies published to date. One practical constraint: PRP plus microneedling is not a DIY option. PRP requires blood draw, centrifugation, and injection by a licensed clinician, and the quality of PRP preparations varies significantly between providers. If you're considering this combination, it belongs in a clinical setting, not at home.
Topical growth factors as a post-needling adjunct
Several studies have tested topical growth factor serums applied after microneedling, using the absorption window that disrupted skin creates. Combination arms outperformed controls in hair density in the available data, and the mechanism is sound: needling opens channels that allow growth factor concentrations in topical serums to reach the dermis at levels they can't achieve on intact skin. The practical limitation is that product quality and active ingredient concentrations vary enormously in this category, and it has far less regulatory oversight than minoxidil. The biological logic is compelling; the product selection is complicated. If you pursue this adjunct, look for published evidence on the specific formulation rather than extrapolating from mechanism alone.
Finasteride and microneedling: honest about the evidence gap
The evidence for combining microneedling with oral finasteride is weaker and less clearly established than for minoxidil. Finasteride works by blocking the conversion of testosterone to DHT, a systemic mechanism that operates independently of the local wound-healing response that microneedling triggers. In theory, these two mechanisms are complementary: finasteride addresses the hormonal driver of miniaturization while microneedling improves the follicular environment and growth factor milieu. In practice, no sufficiently powered trial has directly tested this combination with rigorous controls. If you're already on finasteride and considering adding microneedling, the theoretical rationale is reasonable, but be clear-eyed that you're not working from the same level of evidence as the minoxidil pairing. That doesn't mean don't do it; it means track it carefully so you can assess your own response.
At-home vs. professional microneedling for hair growth: the real trade-offs
Most people who pursue microneedling for hair growth will do at least some of it at home, and that's a realistic starting point rather than a mistake. But the trade-offs between at-home and professional treatment are specific and worth understanding before you choose a device and protocol.
How professional and at-home devices actually differ
Professional dermapens offer adjustable depth settings, consistent perpendicular penetration calibrated to scalp skin thickness, and speed controls suited to larger treatment areas. A trained clinician also applies consistent pressure across the treatment zone, which is harder to replicate with a hand-held roller. At-home dermarollers are fixed-depth, apply oblique rather than perpendicular penetration, and require the user to maintain consistent pressure and coverage across an irregular scalp surface, something most people find difficult to do reliably. The clinical studies showing the strongest benefit primarily used professional devices or closely supervised protocols. That's worth noting without overstating: at-home protocols have shown benefit in some studies, but consistency of delivery is a genuine variable.
The real risks of unsupervised dermarolling
Infection is the most significant added risk of at-home use. Needles that aren't sterilized between sessions, or cartridges used past their effective lifespan, introduce bacteria directly through an open skin barrier. The FDA has specifically flagged home-use microneedling devices as higher infection risk when cartridges are reused or not properly cleaned. Beyond infection, excessive pressure is a common user error: people who aren't seeing results often press harder as compensation, which increases scarring risk and post-inflammatory hyperpigmentation rather than improving outcomes. Track marks, uneven treatment patterns, and contact dermatitis from misapplied topicals are reported more frequently with unsupervised home use than in clinical studies. Across 657 subjects in published clinical studies, no serious adverse events were recorded; in at-home settings, that safety record is harder to replicate without proper technique.
When professional treatment is worth the cost
Active scalp conditions, including seborrheic dermatitis, folliculitis, or psoriasis, require professional assessment before any needling begins, full stop. Treating inflamed or infected scalp skin with a microneedle device spreads bacteria and worsens inflammation rather than triggering a productive healing response. Protocols at 1.2mm depth or higher are also safer in a clinical setting where depth and pressure are controlled precisely. PRP combinations require professional administration regardless of your experience level with at-home tools. If your scalp is currently in good health, your hair loss pattern is well-defined, and you're committed to sterilization and technique, at-home treatment in the 0.5 to 0.75mm range is a reasonable starting point. If any of those conditions don't apply, a professional assessment before starting is the practical move.
Sterile technique and aftercare: the protocol most people skip
The session itself gets most of the attention in how-to guides, but what you do before and after each session determines both safety and efficacy. These steps aren't optional add-ons; they're part of what makes the protocol work.
Pre-treatment preparation
Wash your scalp thoroughly with a gentle, residue-free shampoo before every session. Sebum, product residue, and bacteria on the scalp surface get pushed into the dermis by needle channels, that's how minor contamination becomes a meaningful infection risk. Wipe the device cartridge or roller with 70% isopropyl alcohol before use, and replace or sterilize disposable cartridges regularly per manufacturer instructions. Needle tips dull with repeated use and increase tissue trauma over time without improving penetration. Do not microneedle over active pimples, scabs, inflamed patches, or open wounds anywhere on the scalp, even if they're in an area unrelated to your primary treatment zone. Bacteria introduced anywhere on the scalp can spread through the session regardless of where you begin needling.
What to do (and avoid) in the 5 days after a session
Redness, tenderness, and mild swelling are normal in the 24 to 72 hours following a session and typically resolve within 5 days. Clinicians commonly recommend avoiding heat exposure, hot showers, saunas, and direct sun, for the first 24 hours post-session, as heat increases inflammation in already-disrupted skin. Skip minoxidil for the first 24 to 48 hours as covered above, then resume your normal schedule. Many practitioners also advise avoiding harsh shampoos, sulfates, and fragranced products for at least 48 hours after treatment, since the scalp barrier is compromised and absorbs irritants more readily than it would on an untreated day. Keep the protocol boring and consistent; variability in aftercare creates variability in results that makes it impossible to know what's actually working.
Warning signs that require medical attention
Pustules appearing on the scalp within 48 to 72 hours post-session, pain that worsens after the second day rather than fading, crusting that spreads beyond the treated area, or systemic symptoms like fever are signs of infection. These symptoms require a dermatologist visit, not a wait-and-see approach. Do not attempt to continue your microneedling schedule through an active infection or inflammatory reaction. Restarting sessions before a reaction fully resolves compounds the tissue damage and significantly increases scarring risk. The healing interval exists for a reason, and cutting it short when something has already gone wrong is the fastest path to long-term damage.
Who should skip scalp microneedling entirely
For all the conditions where microneedling and hair growth are linked by evidence, there are specific profiles where it's contraindicated, and several hair loss types where it simply isn't the right tool for the problem.
Medical and skin-condition contraindications
Active scalp infections, folliculitis, and seborrheic dermatitis flares are hard contraindications: microneedling spreads bacteria, introduces pathogens through the skin barrier, and worsens existing inflammation. Pregnancy is a complete contraindication, with no safety data and no clinical justification for use. People on blood thinners or with bleeding disorders face meaningfully increased bruising and prolonged bleeding from needle channels, raising both safety concerns and the practical challenge of assessing a scalp during a session.
Diabetes and other conditions that impair wound healing remove the core mechanism that makes microneedling work: the healing response that produces growth factors depends on the body's ability to mount and complete a proper healing cascade. A history of keloid scarring is also a significant red flag. Repeated skin disruption combined with a known tendency toward abnormal scar formation is not a combination to test on your scalp.
Hair loss types where the evidence is weak or absent
Scarring alopecias, including lichen planopilaris and frontal fibrosing alopecia, involve active inflammation as the mechanism of damage. Needling into fibrotic scalp tissue in an actively inflamed scarring alopecia can accelerate destruction of follicles rather than stimulate them. These conditions require anti-inflammatory treatment, not mechanical stimulation. Telogen effluvium, the stress-related or systemic shedding pattern, has a root cause that is entirely systemic: nutritional deficiency, hormonal change, illness, or severe stress. Microneedling the scalp does not address any of those root causes and is unlikely to produce meaningful benefit. Alopecia areata has some PRP plus microneedling data showing improvement in SALT scores, but the evidence is not strong enough to make scalp needling a first-line recommendation for this immune-mediated condition. If your hair loss doesn't fit the androgenetic alopecia profile, the mechanism that makes microneedling effective may not apply to your situation.
Tracking whether your microneedling hair growth protocol is actually working
Running a protocol for 12 weeks and then deciding whether it worked based on how your hair looks in a bathroom mirror is not a measurement. It's a mood-dependent impression. The most overlooked part of any hair loss treatment is the objective tracking that turns subjective feelings into real data.
Why self-assessment from a camera roll doesn't work
Hair regrowth is slow and millimeter-scale over months. Changes that take 16 weeks to accumulate are invisible between any two casually taken photos, especially when lighting, hair length, styling, and camera angle shift between shots. A photo from a bright bathroom window on a Tuesday and one from overhead lighting on a Saturday are not comparable images, and making treatment decisions based on that comparison is unreliable at best. The mirror test is even worse: perception of hair density shifts with mood, light direction, and how much you want something to be working. A treatment that genuinely moves hair density by 15% over four months is invisible to the mirror because it unfolds too gradually for direct visual perception to track. The only way to detect slow, incremental change is to control for every variable that isn't hair density.
How Folicle turns a microneedling log into structured data
Folicle was built specifically for this problem. The treatment log records each microneedling session with date, needle depth, device, and any post-session reactions, sitting alongside your daily minoxidil or finasteride log in a single timeline. Weekly 5-angle scalp photo sessions auto-align each new image to your baseline frame, so every comparison is genuinely apples-to-apples regardless of how your lighting or angle shifted that week. The Hair Score, a composite 0-to-100 metric aggregating density, coverage, hairline position, hair caliber, and scalp health, gives you one consistent number to track across sessions. At the 12-week mark, you're not asking yourself whether you think it looks better; you're looking at a Hair Score trend line overlaid on your treatment log and seeing whether adding microneedling to your routine moved the score. That is the difference between a trackable routine and a guess.
What to look for at 3, 6, and 12 months
At the three-month mark, realistic early signs include reduced shedding in the treated zone and the first appearance of new, finer hairs at the hairline or crown. Your Hair Score should show an upward trend if the protocol is producing a biological response, even before changes are visible in photos. At six months, you're looking for documentable improvement in density or coverage that holds up in side-by-side photo comparisons taken under the same conditions. This is also the point at which you have enough data to make an informed decision about adjusting frequency or depth. At 12 months, you have a complete dataset: a full year of treatment logs, aligned photo comparisons, and a Hair Score trend that tells you whether microneedling contributed meaningfully to your results. That's also the point at which an exportable timeline from Folicle becomes a useful asset in a dermatologist appointment, replacing a chaotic camera roll with a structured, chronological record.
The bottom line on microneedling for hair growth
Microneedling for hair growth has a real evidence base, but it still needs careful framing. The biological mechanism is well-described, the RCT data is directionally consistent, and the 2025 meta-analysis of 13 trials and 696 patients makes a credible case for its use as an adjunct to minoxidil in androgenetic alopecia. The pooled improvements in hair density and hair diameter are statistically significant, and the safety profile across those trials was comparable to monotherapy. That's a meaningful evidence base for an adjunct treatment, even if it doesn't make microneedling a standalone solution.
The protocol parameters the evidence supports are specific: needle depth in the 0.5 to 1.5mm range (with the counterintuitive finding that 0.6mm outperformed 1.2mm in at least one direct comparison), biweekly to monthly session frequency depending on depth and device type, a minimum 12-week commitment before evaluating results, and a 24-hour gap before applying minoxidil after each session. Anything that deviates significantly from those parameters is moving away from what the evidence actually tested.
The part of the protocol most people skip is the measurement. Whether you use Folicle's tools or another structured method, the goal is the same: replace subjective mirror-checking with repeatable, consistent data that tells you at the 12-week mark whether your Hair Score is moving, at the 6-month mark whether the change is visible in controlled photo comparisons, and at 12 months whether the investment in this routine has been worth continuing. A treatment routine without objective tracking is a routine you are hoping works. Tracking turns it into a decision you can actually make with evidence.
How would you rate this content?
Your feedback helps us improve the quality of our articles
Sources and clinical references
Research on scalp microneedling and hair growth is available in this PMC review.
One randomized, single-observer blinded study compared topical minoxidil plus microneedling with topical minoxidil alone.
A more recent systematic review and meta-analysis summarized randomized trial evidence for microneedling in androgenetic alopecia.
Not medical advice. Do not microneedle over active scalp infection, open wounds, painful inflammation, or unclear hair-loss patterns. Ask a board-certified dermatologist before starting procedures or changing treatment.
Frequently asked questions
Does microneedling help hair growth?
Microneedling has evidence as an adjunct for androgenetic alopecia, especially with topical minoxidil. It is not a guaranteed standalone treatment and should be discussed with a clinician if you have scalp symptoms or unclear hair loss.
How long does microneedling take to show hair results?
Most people need at least 12 weeks before judging early signals, and 4 to 6 months is a more realistic window for visible photo comparisons.
Can I use minoxidil right after microneedling?
Many dermatologist-facing protocols advise waiting about 24 hours after microneedling before applying minoxidil, because broken skin can burn, irritate, and increase absorption.
What needle depth is best for scalp microneedling?
Studies use a range of depths, often around 0.5 to 1.5 mm, but deeper is not automatically better. Device type, scalp tolerance, and clinician guidance matter.
Who should avoid scalp microneedling?
Avoid microneedling over infection, inflamed scalp disease, open wounds, painful lesions, or uncertain diagnoses. Pregnancy, bleeding risk, and poor wound healing also deserve medical advice first.
How should I track microneedling progress?
Log session date, device, depth, reactions, minoxidil timing, and aligned scalp photos. Compare monthly rather than judging from random camera-roll photos.
Is microneedling a replacement for finasteride or minoxidil?
No. Microneedling does not block DHT and should not be treated as a replacement for clinician-recommended therapy. It is usually discussed as an adjunct.
Can Folicle diagnose whether microneedling is working?
No. Folicle helps organize photos, treatment notes, and timelines. It does not diagnose hair loss or tell you which treatment to use.